She Was Told ‘You Might Die’ Right Before Childbirth: A Probe Of Georgia’s Maternal Mortality Crisis

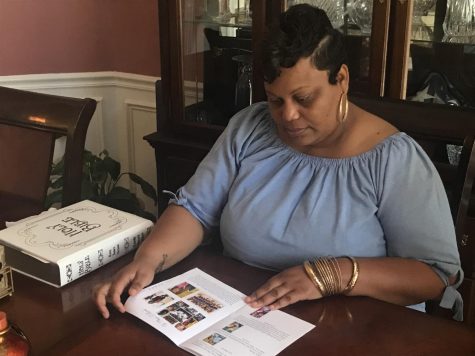
Athena Robinson rushed to the hospital twice in severe pain from her pregnancy with her second child. She was three weeks away from a scheduled cesarean section. Adding to her fears, it was the height of the COVID-19 pandemic last year.
The 32-year-old Fulton County resident was scared for her baby and had sought the best medical care possible. But both times, she said, she was sent home, told that it was just part of ordinary pregnancy discomforts.
Her health quickly deteriorated after returning home. Within two days, her blood pressure soared above 280, a dangerously high level.
“I was in so much pain,” she said. “I couldn’t walk. I couldn’t move. My body literally shut down on me.”
She was whisked away by ambulance. Paramedics worried she would go into shock. But even as her health spiraled out of control, it would be another 12 hours before Robinson would undergo surgery.
A midwife told her doctors would have to put her under anesthesia and pull her out repeatedly to keep her vital signs stable.
“We have to do this so you don’t die,” the midwife told her.
Reflecting on that moment, Robinson said, “You don’t want to hear that right before you’re about to give birth — that you might die.”
‘They were already fearful’
Robinson’s experience is what maternal health experts call a “near miss” — another Georgia mother who nearly died in a state with a disproportionately high maternal mortality rate. The deaths are often the result of health disparities along racial lines.
Black women in Georgia are nearly three times more likely to die during childbirth than white women — a statistic that’s in the forefront of many mothers’ minds as they go into labor, said Dr. Natalie Hernandez, an assistant professor at Morehouse School of Medicine and executive director of the Center for Maternal Health Equity.
“They were already fearful,” she said. “No woman should fear what should be the most beautiful experience of their life for those that want to have a baby.”
Georgia consistently ranks among the bottom 10 states for the number of mothers who die during childbirth. But experts and advocates agree, many of the deaths could have been avoided. According to the Department of Public Health, 70% of Georgia’s maternal deaths from 2012 to 2016 were preventable.
Some experts argue that one of the missing links in combating Georgia’s startling maternal mortality crisis is hearing from the women who barely made it out of labor alive.
Hernandez is working on a grant-funded research study focused on the stories of women like Robinson. The goal, she said, is to dissect the root causes and issues behind maternal deaths that are largely preventable, especially among women of color.
“We’re talking to women who have had these complications and they’re alive to talk about those situations,” Hernandez said. “But a lot of women don’t get an opportunity to really tell their stories.”
Biases ‘affect your health’
Researchers in Georgia, New Jersey, Louisiana and the District of Columbia — the areas with the highest maternal mortality rates in the country — are setting out to document the experiences of mothers who suffered severe pregnancy complications.
Hernandez said of the interviews already conducted, many mothers were low-income, on Medicaid and, like Robinson, almost died of preeclampsia.
Advocates say, in the South in particular, the health care system is permeated by a legacy of racism and discrimination that causes doctors to treat women of color differently than their white counterparts.
And those implicit biases sometimes have fatal outcomes.
Ky Lindberg, executive director for nonprofit organization Healthy Mothers, Healthy Babies, said for women of color going through pregnancy, racism can impact their outcome regardless of income.
“It doesn’t matter what your pocketbook looks like or your scale of influence,” she said. “If those biases exist, they exist and it can affect your health.”
Lindberg herself almost died during the birth of her first child after doctors gave her medications that caused her to have eclampsia.
But women who experienced near miss situations, shouldn’t have to relive their trauma and tell their stories to receive quality care, she said.
“We should just automatically give people the type of care that they deserve,” she said. “…I just think aside from storytelling, we just need to do what’s right.”
Georgia advocates have been pressing lawmakers for policy changes to help curb the state’s high rate of maternal deaths.
Last session, legislators extended postpartum Medicaid coverage from the previous 60-day period to six months — although stakeholders are pushing for coverage to stretch a full year.
“This hasn’t been a new issue,” Lindberg said. “But I will say it’s a refreshed issue. There’s a lot more energy being put into solving this. We have made some strides over the last several years.”
The state’s Maternal Mortality Review Committee — which reviews each case — has also been under pressure to speed up its process. As of August, the committee had reviewed cases through 2018.
Members of the committee, formed in 2013 by lawmakers, said that the review of cases has been streamlined and improved from earlier, clunkier processes.
Katie Kopp, senior manager in the office of women’s health for the state, said that the Centers for Disease Control and Prevention has told the committee to catch up on its backlog of cases.
“We’re just getting to that point,” she said. “We’ve also been able to review them more thoroughly than we ever have before.”
Dr. Chad Ray, the medical director for perinatal services at Augusta University Medical Center and member of the state’s committee, said that while it’s still vulnerable to inaccuracies, the process has been carefully curated to be the best it can be.
“I think what is so critically important here is what separates Georgia and other states that domaternal mortality review is that we actually have a process by which to have had the best data that we can have,” he said.
But there’s one finding in the data that’s always been consistent, he said: Black women are at higher risk of death.
“The million-dollar question is why?” he said. “And it’s the billion-dollar answer. It’s not easy. It’s not simple. It’s multifactorial. It’s so complicated that the greatest minds in my field will not figure it out probably in our lifetimes. But it is consistent.”
Robinson said many Black women don’t know where to go to get help.
After she gave birth to her second child, she was expected back at work a week later but was eventually let go from her tech support jobfor medical reasons.
While her body slowly healed, the toll the experience took on her mental health still lingers.
“It’s scary that you don’t know if you’re going to make it out alive,” she said. “It’s hurtful.”
When she looks at her healthy 1-year-old boy, Adonai, she said, the pain washes away. But she also still feels the sting of what might have been.
“He’s walking; he’s laughing; he’s playing,” Robinson said. “But still sometimes looking at him, it’s like, ‘Wow, one of us could have not been here.’”
She added, “I am surprised I am still alive — really.”
Listen to the story here.